Late surgery for Cerebral Palsy
Late surgery for Cerebral Palsy
As we explained in a previous article on Cerebral Palsy and Early Surgery, a multidisciplinary approach involving all specialists (neurologists, physiotherapists, gastroenterologists and even dentists) is always necessary for patients with cerebral palsy (CP). Each of them can, indeed, make a fundamental contribution within their discipline, both from the diagnostic and therapeutic point of view.
The ideal option for patients affected by CP, who in many cases know that they will have to undergo orthopaedic surgery even more than once in their lifetime, is to intervene as soon as possible, when the children are still growing and the margins for improvement are greater.
But of course, there are also family, health and psychological aspects that need to be taken into account, that need to be respected and that can delay the time of surgery. There are also problems that arise later and that must be addressed when they occur (comorbidities such as lung problems, gastroenterological nutrition).
It should be borne in mind that a late intervention is often more complex and even longer. These factors can expose the patient to greater risks and complications.
The most common types of late surgery are:
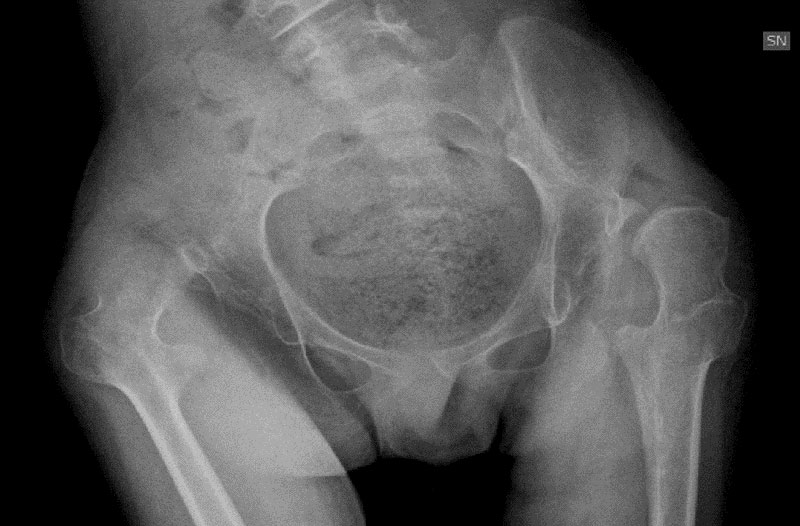
- Osteotomy of the proximal femur to center the femur head within the acetabulum, which sometimes includes reconstruction of the acetabulum itself.

Pelvic and Proximal Femoral Osteotomies Pre – post surgery and follow up (2 years later)
- The pan release of all muscles of the thight that is performed in the most severe cases where the femoral head is completely deformed and the hip joint can no longer be reconstructed.

- resection of the femoral head, which is performed in the most serious cases of deformity of the femoral head and the acetabulum
- osteotomy of knee extension in cases of fixed deformity of the flexing condyles
- transfer of tibial tubercle distally for realignment of the patella
- the total reconstruction of the foot: in the case of serious deformities of the foot, even inveterate (i.e. by now consolidated and difficult to correct). The logic is to reconstruct the foot in a total way by realigning the various portions of the foot to allow a better static and dynamic balance of the body.
Conclusions
As explained in the article on Early and “Tailor-made” surgery for Cerebral Palsy it is always better, where possible, to prefer early interventions of minimally invasive surgery.
This is because, unlike in the past, children can undergo surgery at 5 or 6 years of age and at this age, the recovery time is faster and involves fewer complications.
In addition, the growth potential of small patients’ joints can also be exploited.
Orthopaedic surgery, however, offers effective solutions even after the patients have completed the growth phase, especially to intervene in the most serious cases and improve, where possible, the clinical and living conditions of these patients, alleviating situations of discomfort or pain.